When OR ventilation falls short, the consequences are real: slower pathogen removal, compromised sterility, staff exposure to waste anesthetic gases, and direct risk to patient safety. Despite this, OR HVAC systems remain among the most under-maintained in healthcare facilities, often receiving attention only after a compliance failure surfaces during accreditation review.
This guide covers why OR air exchange rates matter, what standards govern them, what maintenance looks like in practice, and how to recognize warning signs before they become patient safety events.
Key Takeaways
- ASHRAE 170 requires a minimum of 20 total ACH (4 outdoor) during occupied OR use
- Filtration must meet MERV 16 minimum; HEPA is required at terminal devices for orthopedic, transplant, neurosurgery, and burn procedures
- Positive pressurization of at least +0.01 in.w.g. must be maintained to prevent contaminant ingress
- Preventive and corrective maintenance are both required; reactive-only approaches leave compliance gaps and put patients at risk
- ASHRAE 170 permits unoccupied ACH setbacks to 5–6 per hour, cutting fan energy without sacrificing compliance
Why Proper Air Exchange in Operating Rooms Is Critical for Infection Control
Operating rooms face contamination risks that few clinical environments match. Open surgical wounds create a direct infection pathway, patients are often immunocompromised, and staff movement, instruments, and anesthetic gases continuously introduce particulates. Without adequate air exchange, that particulate load builds — directly at the surgical site.
ACH Rates and Pathogen Removal
ACH rates translate directly into contaminant removal speed. According to CDC data, assuming an empty room and ideal air mixing:
- At 15 ACH: 99% contaminant removal takes approximately 18 minutes
- At 20 ACH: 99% contaminant removal takes approximately 14 minutes
During a multi-hour procedure, those four minutes represent dozens of additional removal cycles — each one reducing the probability of airborne pathogen accumulation at the surgical site.
Airflow Direction and Pressurization
Direction matters as much as volume. Air must flow from the clean surgical zone outward toward adjacent less-clean areas. The CDC specifies a minimum pressure differential of 0.01 in.w.g. (2.5 Pa) between the OR and adjacent corridors, maintained continuously during occupied use. When this differential drops — even briefly — unfiltered corridor air can infiltrate the sterile field.
The Evidence on Air Quality and Surgical Site Infections
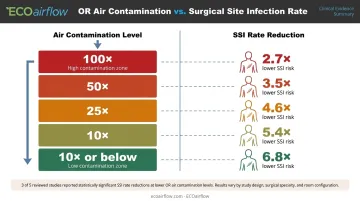
The relationship between OR air quality and surgical site infections (SSIs) is well-documented in the literature, though the science is nuanced. A 2025 systematic review in the Journal of Hospital Infection found that 3 of 5 included studies showed a significant correlation between intra-operative air contamination and SSI incidence. Historical data cited in the review found that 10-fold to 100-fold differences in air contamination levels correlated with 2.7-fold to 6.8-fold reductions in SSI rates — a meaningful spread for infection control teams.
Temperature and Humidity
OR air quality extends beyond particle filtration. The CDC specifies:
- Temperature: 68–73°F (20–23°C)
- Relative humidity: 30–60%
These ranges are not arbitrary. They inhibit microbial growth, support patient thermoregulation during open procedures, and prevent condensation that can harbor contaminants on surfaces and ductwork.
Together, ACH rates, pressurization, and environmental parameters form an interdependent system — a failure in any one element can compromise the others.
Operating Room Air Exchange Standards and Regulatory Requirements
Three primary frameworks govern OR ventilation in the United States. Compliance teams, facilities managers, and specifying engineers each need to know where these standards overlap — and where they diverge.
ANSI/ASHRAE/ASHE Standard 170
Standard 170 (current edition: 2025) is the most widely adopted U.S. benchmark for healthcare facility ventilation. Its OR-specific requirements are precise:
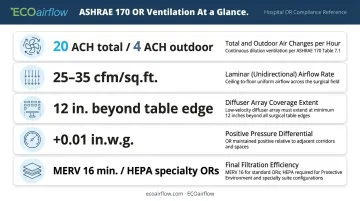
- Minimum 20 total ACH, with at least 4 ACH of outdoor (fresh) air
- Unidirectional downward laminar airflow at 25–35 cfm per sq. ft.
- Primary supply diffuser array must extend at least 12 inches beyond the surgical table footprint on each side
- Positive pressure of at least +0.01 in.w.g. maintained at all times during occupied use
- Recirculating room HVAC units are not permitted in ORs
Filtration requirements under the 2021 update pathway specify a minimum of MERV 16 for general OR Filter Bank No. 2 — an increase from the prior MERV 14 threshold. For ORs designated for orthopedic, transplant, neurosurgery, or burn procedures, HEPA filters (99.97% efficiency at 0.3 microns) are required at air terminal devices.
ACH Setback Provisions
Standard 170 doesn't require full ventilation rates around the clock. When ORs are unoccupied, ASHRAE 170 permits ACH reduction to maintain energy efficiency, provided pressure relationships between adjacent rooms are preserved. ASHE's OR airflow setback guidance describes a typical setback target of 5 ACH during unoccupied periods. Critically, time-delay controls must prevent setback for at least 20 minutes after a space becomes unoccupied, allowing contaminant levels to reach approximately 90% reduction before turndown begins.
CDC Guidelines and FGI Standards
The CDC's Guidelines for Environmental Infection Control in Health-Care Facilities reinforce ASHRAE 170's parameters with additional infection control context. AIA/FGI Guidelines govern facility design and construction, applying primarily during new construction and renovation. Both are typically adopted by reference by state health departments and accreditation bodies.
Key roles each standard plays:
- CDC Environmental Infection Control Guidelines — reinforce ASHRAE 170's ventilation parameters with pathogen-specific context for ongoing operations
- AIA/FGI Guidelines — govern facility design and construction; apply primarily during new builds and renovation projects
- State health departments and accreditation bodies — typically adopt both standards by reference, making them effectively mandatory
LEED and ASHRAE 189.3
ANSI/ASHRAE/ASHE 189.3 covers design, construction, and operation of sustainable healthcare facilities. LEED Healthcare's Enhanced Indoor Air Quality Strategies credit (up to 2 points) rewards facilities that go beyond baseline ventilation codes through higher-performance filtration strategies, giving facilities a concrete financial and reputational reason to invest in advanced filtration beyond the minimum.
Types of Maintenance for OR Air Exchange Systems
OR HVAC maintenance is not a single task. It is a layered system of scheduled, reactive, condition-based, and periodic deep-service activities — each serving a distinct compliance and performance function.
Preventive / Routine Maintenance
Scheduled preventive maintenance keeps the OR within compliance thresholds between formal inspections. Core tasks include:
- Regular filter inspection and replacement per manufacturer schedule
- ACH verification through airflow measurement
- Pressure differential gauge checks
- Diffuser array and return/exhaust grille cleaning
- Duct integrity inspection
Filtration choice directly affects how often preventive tasks are needed. ECOairflow's M-Series Hybrid (MERV 13–16A, Appendix J certified, ASHRAE 170 / CSA Z317.2 compliant) maintains a nearly constant pressure drop of 0.09–0.38 in.w.c. at operating velocities. Unlike traditional bag filters, it doesn't progressively load — reducing pressure-alarm-driven interventions and cutting HVAC fan energy by up to 54% versus a MERV 8 + MERV 14 bag filter train in an independent 12-week hospital study.

Corrective / Reactive Maintenance
Corrective maintenance is triggered by system failures — not scheduled intervals. Common triggers in OR environments include:
- Pressure alarms indicating loss of positive pressurization
- ACH dropping below the 20 ACH minimum
- Filter breakthrough or failure
- Diffuser blockage
- Unexpected air handler failures
Relying on corrective maintenance alone is especially dangerous in ORs. Downtime directly affects patient scheduling. A documented compliance failure — ACH or pressure outside required parameters with no recorded corrective response — can trigger accreditation issues or procedure cancellations under Joint Commission EC.02.05.01.
Predictive / Condition-Based Maintenance
Predictive maintenance uses continuous monitoring to trigger action only when performance actually degrades:
- Pressure differential sensors detect pressurization loss in real time
- Airflow monitors integrated with BAS track ACH continuously
- Filter loading indicators signal replacement before performance drops below threshold
ASHE recommends interfacing OR room scheduling systems with the building automation system (BAS) to automate ACH ramp-up before procedures begin and detect setback failures immediately. This cuts unnecessary maintenance costs and closes the compliance gaps that fixed-schedule service routinely misses.
Major / Overhaul Maintenance
Major servicing events — typically required after significant facility renovations or on a periodic cycle — include:
- Full HVAC unit inspection and coil cleaning
- Ductwork pressure testing and leak detection
- Air handler replacement where aging units are identified
- Full system recommissioning with Testing, Adjusting, and Balancing (TAB) verification
ASHE guidance specifies annual supply-air and ACH verification by balometer as a minimum. Overhaul events are also the appropriate time to upgrade filtration to current standards — facilities still operating MERV 14 filters should transition to MERV 16 (or HEPA at terminal devices per room classification) to meet the 2021 ASHRAE 170 update.
Signs Your OR Air Exchange System Needs Maintenance
Infection control officers, facilities managers, and OR directors need to identify performance degradation before it becomes a compliance event. These are the indicators to watch.
Performance or Output Changes
The most critical performance indicators are:
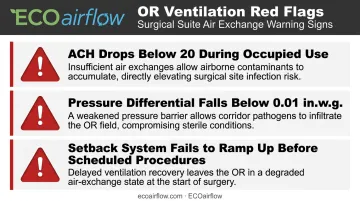
- ACH dropping below 20 during occupied use — requires immediate investigation
- Pressure differential falling below 0.01 in.w.g. — loss of positive pressurization compromises the sterile field
- Setback system failing to ramp back up before scheduled procedures
These should be detected by continuous monitoring systems. Manual spot checks alone are not sufficient for sustained ASHRAE 170 compliance.
Visible Wear and Physical Indicators
Physical signs that warrant immediate inspection:
- Visibly soiled or loaded filters
- Obstructed diffuser grilles or blocked return vents
- Condensation or moisture on ductwork (humidity control failure)
- Nuisance pressure alarms suggesting seal degradation or damper malfunction
Each of these compromises either filtration efficiency or airflow patterns — the two variables that determine OR air quality.
Increased Energy Consumption
Rising energy draw from air handling units — with no corresponding change in occupancy or procedure volume — signals filter loading, coil fouling, or duct leakage. All three reduce airflow efficiency and can cause ACH to fall below required levels without triggering pressure alarms.
DOE data shows dirty or loaded filters can increase HVAC energy consumption by 5–15%. In hospital air handlers running continuously at high ACH rates, that penalty compounds quickly.
Traditional bag filters show 60%+ increases in fan power demand as they load over a standard 12-week service cycle — a well-documented performance degradation pattern in high-ACH commercial air handling applications.
OR Air Exchange Maintenance Schedule: General Guidelines
Maintenance intervals vary based on OR usage intensity, filtration technology, local regulatory requirements, and accreditation standards. The following framework reflects guidance from ASHE, the Joint Commission, and standard industry practice.
| Frequency | Tasks |
|---|---|
| Daily / Per-Use | Pressure differential confirmation; temperature and humidity log review; visual inspection of diffusers and return grilles |
| Weekly | Airflow spot-checks; filter loading visual inspection; alarm system testing |
| Monthly / Quarterly | Formal ACH measurement via balometer; filter replacement or pad inspection per manufacturer schedule; grille cleaning |
| Annual / Overhaul | Full system recommissioning; ductwork inspection; HEPA filter integrity testing where applicable; BAS interface calibration |

Notes on adjusted scheduling:
- Low-use ORs: Setback programs demand documented ramp-up verification before each procedure — confirm the system has restored 20 ACH before the patient enters
- High-volume / trauma ORs: Near-continuous occupied ACH accelerates particulate loading; increase filter inspection frequency accordingly
- Documentation: Joint Commission EC.02.05.01 treats undocumented maintenance the same as maintenance not performed — every task requires a record
ASHE requires annual balometer verification of supply air quantity and total ACH. HEPA filters require challenge testing at installation to confirm seal and media integrity, with follow-up testing built into the preventive maintenance plan.
Conclusion
OR air exchange maintenance is a patient safety function, not a facilities management afterthought. Compliance with ASHRAE 170, CDC guidelines, and Joint Commission standards depends on consistent, documented, multi-layered maintenance — from daily pressure checks to annual system recommissioning.
Selecting the right filtration technology is what makes that compliance sustainable. ECOairflow's M-Series Hybrid electronic air filtration system meets ASHRAE 52.2 MERV 16A Appendix J certification, ASHRAE 170 / CSA Z317.2 compliance, and UL 2998 Zero Ozone verification. It maintains full rated MERV performance powered, unpowered, and under Appendix J conditioning.
For hospital specifying engineers and facility procurement teams, full submittal documentation and compliance data are available upon request at 1-877-347-3569 or sales@ecoairflow.com.
Frequently Asked Questions
What is the recommended air changes per hour in the operating room?
ASHRAE 170 and CDC guidelines require a minimum of 20 total ACH during occupied use, with at least 4 of those being outdoor air. Some facilities operate at 20–30 ACH depending on cooling loads, procedure type, and system design.
What is 1 air exchange per hour?
One ACH means the total volume of air in a room is replaced once per hour. At that rate, 99% contaminant removal takes over two hours — which is why ORs require 15–20+ ACH to maintain a clinically safe environment during active procedures.
What is the minimum filtration efficiency required for OR HVAC systems?
ASHRAE 170 (2021 update pathway) requires a minimum of MERV 16 for general OR filtration. HEPA filters (99.97% at 0.3 microns) are required at air terminal devices for orthopedic, transplant, neurosurgery, and burn procedures.
What is positive pressurization in an OR and why does it matter?
Positive pressurization means the OR is maintained at higher air pressure than adjacent corridors (minimum 0.01 in.w.g.), causing air to flow outward and preventing unfiltered air from entering the sterile surgical zone.
Can air be recirculated in an operating room?
No. Recirculating room HVAC units are not permitted in ORs under ASHRAE 170 or CDC guidelines. All supply air must be centrally filtered and delivered through the primary diffuser array, with exhaust routed to return or exhaust grilles.
How often should OR HVAC filters be inspected or replaced?
Filter inspection should occur at least monthly, with replacement determined by filter loading, manufacturer specifications, and usage intensity. High-efficiency electronic filters with low, stable pressure drop may support longer service intervals than standard pleated or bag filters, reducing maintenance disruptions in active clinical environments.


