
Introduction
Hospitals run on precision — precise dosing, precise procedures, precise infection controls. Yet one of the most consequential variables in patient outcomes is invisible: the air moving through HVAC ducts, circulating through operating rooms, and flowing past immunocompromised patients who have no defense against what's inside it.
Most hospital attention goes to surface sanitization, surgical protocols, and staffing ratios. But poor air quality contributes directly to healthcare-acquired infections, occupational illness among clinical staff, and regulatory non-compliance — with consequences that rarely get traced back to the air.
What follows breaks down what hospital IAQ means in practice, why it has measurable consequences for patient outcomes and facility costs, and what effective management actually requires.
Key Takeaways
- 1 in 31 U.S. hospital patients has at least one HAI on any given day — and a meaningful share are airborne or ventilation-linked
- Poor hospital IAQ directly affects infection rates, staff sick days, CMS reimbursement, and OSHA compliance
- Each hospital zone — operating rooms, ICUs, isolation rooms, patient wards — requires its own filtration standard
- ASHRAE 170 mandates MERV 14 for most clinical areas and MERV 16 for general operating rooms — not MERV 13
- Reactive remediation always costs more than consistent filtration and monitoring
What Is Indoor Air Quality in Hospitals?
Hospital IAQ refers to the condition of air inside a healthcare facility — specifically the presence, concentration, and movement of airborne contaminants that affect the health and safety of patients, staff, and visitors.
In practice, hospital air is far more complex than commercial or residential air. Healthcare environments generate a unique mix of hazards at the same time:
- Biological pathogens from patients — bacteria, viruses, fungal spores
- Chemical gases from anesthesia and sterilization — waste anesthetic gases (WAGs), formaldehyde, glutaraldehyde
- Fine particulate matter from surgical procedures — including surgical smoke containing viable bacteria, viruses, and cellular material
- Outdoor pollutants entering through ventilation systems — PM2.5, ozone, traffic-related ultra-fines
Each of these contaminant classes moves through shared HVAC infrastructure, crossing zone boundaries when pressure differentials fail or filters underperform. A contamination event in one zone can propagate through the ventilation system before anyone identifies a problem.
That propagation risk is what elevates hospital IAQ beyond a comfort consideration. Infection rates, patient recovery speed, staff absenteeism, and regulatory compliance standing all tie directly to air quality — making it a clinical and operational priority that belongs at the top of any facility manager's agenda.
Why Hospital IAQ Matters: Key Advantages of Getting It Right
The advantages of strong hospital IAQ management show up in traceable, measurable outcomes — infection rates, patient satisfaction scores, staff sick days, regulatory audits, and energy costs. Here is where each advantage is most consequential.
Reduced Healthcare-Acquired Infections and Better Patient Outcomes
According to the CDC, about 1 in 31 U.S. hospital patients has at least one HAI on any given day, with an estimated 687,000 HAIs and 72,000 deaths occurring in U.S. acute-care hospitals in 2015. The direct medical cost to U.S. hospitals runs between $28.4 billion and $45 billion annually, depending on the inflation adjustment method used.
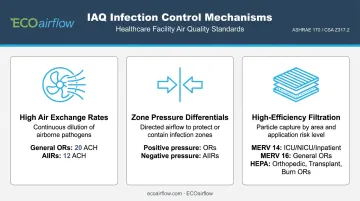
Airborne transmission is one recognized pathway — particularly in zones where patients are most vulnerable and air exchange is most critical. Properly maintained IAQ systems address this through three mechanisms:
- High air exchange rates — general ORs require 20 total ACH; AIIRs require 12 ACH for new construction
- Zone pressure differentials — positive pressure in ORs, negative pressure in airborne infection isolation rooms (AIIRs)
- High-efficiency filtration — ASHRAE 170-2025 specifies MERV 14 for ICUs, NICUs, and general inpatient rooms; MERV 16 for general ORs; and HEPA for orthopedic, transplant, and burn ORs
The financial stakes extend beyond direct treatment costs. CMS does not reimburse hospitals for many HACs (hospital-acquired conditions) not present on admission — meaning a ventilation failure that contributes to a surgical site infection can translate directly into lost revenue. Hospitals in the worst-performing quartile for HAI rates also face a 1% payment reduction under the Hospital-Acquired Condition Reduction Program (HACRP).
The patients most at risk are the ones hospitals can least afford to compromise: post-surgical patients, ICU and NICU patients, and immunocompromised patients such as bone marrow transplant recipients, for whom Aspergillus exposure — linked to contaminated HVAC systems — can be fatal. A published outbreak investigation documented six Aspergillus infections in surgical patients over 12 days, traced to moisture and contamination in ductwork insulation downstream of final filters. No additional cases occurred after HVAC remediation.
KPIs impacted: HAI rates, patient recovery time, readmission rates, HCAHPS satisfaction scores, CMS reimbursement standing
Staff Health, Safety, and Operational Continuity
Healthcare workers face daily exposure to airborne hazards that most professions never encounter. Three categories carry the highest risk:
Waste anesthetic gases (WAGs): A 2026 systematic review and meta-analysis found that healthcare workers exposed to inhalational anesthetics had an odds ratio of 1.29 for spontaneous abortion, rising to 1.56 for high-exposure occupations. OSHA has no established PEL for WAGs; NIOSH recommendations are the primary guidance.
Formaldehyde: OSHA's permissible exposure limit is 0.75 ppm as an 8-hour TWA, with a 15-minute STEL of 2 ppm and an action level of 0.5 ppm. The NTP classifies formaldehyde as a known human carcinogen.
Surgical smoke: NIOSH estimates 500,000 healthcare workers are exposed annually. A 2022 systematic review confirmed surgical smoke can contain bacteria, viruses, HPV and HBV DNA, blood and tissue particles, and viable tumor cells — yet in a NIOSH survey, only 15% of respondents reported always using local exhaust ventilation during electrosurgery.
Hospitals operating in environments with inadequate chemical exposure controls are at risk of OSHA violations. Glutaraldehyde exposure has been documented to cause symptoms at concentrations as low as 0.005–0.050 ppm, and OSHA guidance notes cases where affected healthcare workers left their jobs due to dermatitis.
The operational consequence is direct: a department short-staffed due to respiratory illness or chronic occupational exposure creates cascading risks to patient care quality and emergency responsiveness.
KPIs impacted: Staff sick days, occupational illness rates, OSHA compliance status, nurse-to-patient ratios during illness events
Regulatory Compliance, Financial Performance, and HVAC Efficiency
Hospital IAQ is governed by ANSI/ASHRAE/ASHE Standard 170-2025 (Ventilation of Health Care Facilities), ASHRAE 62.1 (general ventilation design), and ASHRAE 52.2 (filter efficiency testing methodology). Compliance is both a legal requirement and a differentiator for accreditation and funding.
HVAC accounts for nearly half of total hospital energy use, according to DOE's Hospital Energy Alliance — because healthcare facilities require substantial outdoor air intake and continuous high-ACH ventilation. Filter selection directly affects how much of that energy goes to moving air against resistance.
A standard ASHRAE 170-compliant MERV 8 pre-filter plus MERV 14 bag filter configuration imposes a pressure drop of 0.6–1.2 in.w.g.. That resistance escalates by 60% or more as filters load over a 12-week cycle, increasing fan energy demand. ECOairflow's M-Series Hybrid (Appendix J certified to MERV 14A and 16A, using Electronic Polarization Technology) operates at 0.13–0.37 in.w.c. and holds a nearly constant pressure drop throughout the pad's service life.
Independent 12-week testing on identical air handlers documented a 54% reduction in fan power consumption compared to the traditional two-bank hospital filter train.
On the reimbursement and sustainability side, several financial levers tie directly to IAQ performance:
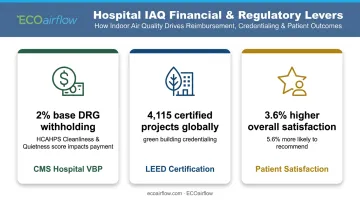
- CMS Hospital VBP: Funded through a statutory 2% reduction to base DRG payments; HCAHPS through FY2026 includes a combined Cleanliness and Quietness score — IAQ affects that score, and that score affects payment
- LEED certification: As of March 2026, 4,115 LEED-certified and registered healthcare projects exist globally
- Patient satisfaction lift: Research in the Journal of Green Building found green hospitals had 3.6% higher overall patient satisfaction, with patients 5.6% more likely to recommend them
KPIs impacted: HVAC energy costs, LEED certification status, HCAHPS scores, regulatory audit outcomes, ASHRAE 170 compliance, filter lifecycle costs
What Happens When Hospital IAQ Is Ignored
The consequences of neglected IAQ management rarely announce themselves as a single event. They compound.
Common failure patterns include:
- An infection outbreak spreads through shared HVAC pathways before the source is identified
- Staff respiratory complaints are treated individually rather than traced to a systemic ventilation failure
- A regulatory inspection uncovers non-compliance that proactive monitoring would have caught months earlier
The financial exposure is concrete:
- HAI costs: $28.4–$45 billion annually to U.S. hospitals; SSIs alone add more than $20,000 per admission and 9.7 extra hospital days
- CMS payment risk: HAC nonpayment, HACRP 1% penalty, and VBP 2% withholding each operate independently — a single poorly managed HAI rate can trigger all three
- OSHA enforcement: Hospitals with inadequate chemical exposure controls face violations, fines, and enforcement proceedings for formaldehyde, glutaraldehyde, and related hazards
Reactive remediation — replacing contaminated HVAC components, responding to infection outbreaks, managing violation proceedings — consistently costs more than a proactive filtration and monitoring program. The Aspergillus outbreak example above required full air-handling system remediation; no additional cases occurred afterward, but the six preceding infections were already on the record.
How to Get the Most Value from Hospital IAQ Management
Effective hospital IAQ management must be zone-specific. Operating rooms, isolation rooms, ICUs, emergency departments, and waiting areas each carry different contamination profiles, different patient vulnerability levels, and different ASHRAE 170 requirements. Uniform facility-wide treatment ignores those differences.
| Hospital Zone | Pressure | Total ACH | Minimum Filtration |
|---|---|---|---|
| General operating room | Positive | 20 | MERV 16 |
| Orthopedic/transplant/burn OR | Positive | 20 | HEPA |
| ICU / critical care | — | 6 | MERV 14 |
| NICU | Positive | 6 | MERV 14 |
| Airborne infection isolation room | Negative | 12 | MERV 14 |
| Protective environment room | Positive | 12 | HEPA |
| General inpatient room | — | 4 | MERV 14 |
Source: ASHRAE/ASHE Standard 170 addenda; verify against 170-2025 for current construction.
Filtration Is the Backbone
Filter selection is often underweighted — not just for infection control, but for energy performance. The assumption that MERV 13 is sufficient for most hospital zones is not supported by current ASHRAE 170 specifications. Most clinical areas require MERV 14 or higher, with general ORs at MERV 16 and specialized ORs requiring HEPA.
Meeting those thresholds typically forces a trade-off: higher filtration grades increase filter resistance, which drives up fan energy costs. ECOairflow's M-Series Hybrid addresses exactly this trade-off. It is Appendix J certified to MERV 13A–16A and maintains its full rated MERV performance whether powered or unpowered — a critical distinction during power events in medical treatment rooms.
Independent testing documents 74.73% PM0.1 ultra-fine particle capture, compared to 49.19% for HEPA under controlled conditions. For Protective Environment Rooms, it replaces the MERV 8 pre-filter and MERV 14 bag filter stages in front of the HEPA terminal filter, eliminating the two-bank pressure penalty while maintaining compliance.
IAQ Outcomes Need Ongoing Review
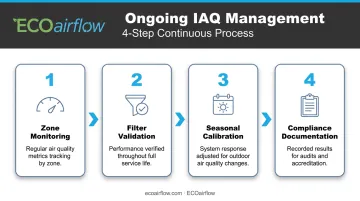
Installation is not management. Effective hospital IAQ requires:
- Regular monitoring of air quality metrics by zone
- Validated filter performance through service life (not just at installation)
- Calibrated system response to seasonal changes in outdoor air quality
- Documented results for compliance, accreditation, and audit purposes
Each of those steps compounds in value when done consistently — and creates defensible documentation when a regulatory inspection or infection event requires accountability.
Conclusion
Hospital IAQ carries direct consequences for patient survival, staff health, and institutional standing — making it a clinical and financial priority, not just a facilities checkbox.
The gains from strong IAQ management — cleaner air, lower infection rates, reduced energy costs, steadier compliance — compound over time. That compounding only happens when filtration, ventilation, and monitoring are treated as continuous operational priorities, not one-time infrastructure decisions.
Frequently Asked Questions
What is indoor air quality in hospitals?
Hospital IAQ refers to the condition of air inside healthcare facilities — covering the concentration of pathogens, chemical compounds, fine particles, gases, and other contaminants that affect the health and safety of patients, staff, and visitors. It is managed through ventilation design, pressure differentials, and high-efficiency filtration across zone-specific requirements.
Can poor indoor air quality in hospitals make you sick?
Yes. Poor hospital IAQ is directly linked to healthcare-acquired infections, respiratory illness, headaches, and long-term occupational health effects. Immunocompromised patients face the greatest risk from airborne pathogens, while staff dealing with daily exposure to surgical smoke, formaldehyde, or waste anesthetic gases bear significant occupational health consequences.
How clean is the indoor air in hospitals?
Air cleanliness varies significantly by zone and facility. Well-maintained hospitals with proper pressure differentials and zone-appropriate filtration can achieve very high air quality. Even modern facilities can have IAQ issues, though, when filtration systems are outdated, filters are improperly maintained, or ventilation rates fall below ASHRAE 170 requirements.
Is poor indoor air quality in hospitals an OSHA violation?
OSHA establishes permissible exposure limits for specific airborne compounds, including formaldehyde (0.75 ppm 8-hour TWA). Hospitals that fail to control employee exposure to these substances within legal limits can face OSHA violations, fines, and enforcement actions. NIOSH also publishes recommended exposure limits for compounds like glutaraldehyde and WAGs, where no OSHA PEL currently exists.
What MERV rating is recommended for hospital air filters?
ASHRAE/ASHE Standard 170 requires MERV 14 for most clinical areas — including inpatient rooms, ICUs, NICUs, and AIIRs — and MERV 16 for general operating rooms. Specialized ORs (orthopedic, transplant, burn, neurosurgery) require HEPA. The "A" suffix (MERV 14A, MERV 16A) denotes Appendix J-conditioned performance — the rating must hold across the filter's service life, not just at installation.
What are the main sources of air pollution in hospitals?
Key sources include airborne pathogens from patients, waste anesthetic gases from operating rooms, chemical vapors from disinfection and sterilization processes, surgical smoke from electrosurgical procedures, outdoor pollutants entering through ventilation systems, and particulate matter from high foot traffic and routine cleaning activities.


