Key Takeaways
- Healthcare HVAC must manage pressure differentials, pathogen containment, humidity, and filtration simultaneously — not just thermal comfort
- ASHRAE Standard 170-2025 governs room-specific requirements; compliance begins before procurement, not after
- Filter selection requires matching MERV rating to system CFM and static pressure capacity — rating without system fit wastes both money and airflow
- Electronic filtration alternatives can deliver MERV 14A–16A performance with up to 54% less fan power than conventional MERV 8 pre-filter + MERV 14 bag filter configurations
- Every maintenance activity requires documentation — inspectors treat incomplete records as compliance failures, regardless of physical filter condition
What Makes Healthcare HVAC Different from Standard Commercial Systems
Walk into any office building and the HVAC system has one primary job: keep people comfortable. Healthcare demands far more.
A hospital's air system must manage all of the following — at the same time, across dozens of functionally distinct room types that may share a single floor plan:
- Air cleanliness and particulate filtration
- Infection containment and pressure isolation
- Humidity control within clinical tolerances
- Room-to-room pressure differentials
- 24/7 uninterruptible operation with no acceptable downtime
The Occupant Diversity Problem
No single default setting works across a hospital population. The same facility houses:
- Newborns and elderly patients with developing or declining immune function
- Surgical patients in sterile recovery environments
- Severely immunocompromised individuals in protective environment rooms
- Infectious isolation patients whose air must not mix with the corridor
- Healthy clinical staff moving between all of these zones
The environmental sensitivity spectrum is enormous. A humidity range that's acceptable in an administrative wing may be clinically dangerous in an operating room.
Multi-Zone Complexity
The table below shows how sharply requirements diverge across just a few adjacent room types, per ANSI/ASHRAE/ASHE Standard 170-2025:
| Room Type | Pressure | Total ACH | Filtration |
|---|---|---|---|
| Operating Room | Positive | 20 minimum | MERV-16 |
| Airborne Infection Isolation Room | Negative | 12 minimum | MERV-14 supply |
| Protective Environment Room | Positive | 12 minimum | HEPA supply |
| General Exam/Observation | Neutral | 4 minimum | MERV-7 minimum |
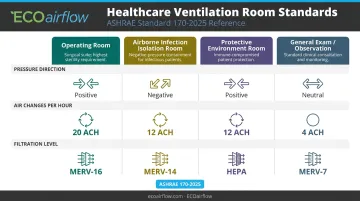
These rooms may sit adjacent to each other. Each requires a different pressure relationship, air change rate, and filtration tier.
The Uptime Requirement
Standard commercial buildings reduce HVAC output overnight. For most critical healthcare zones, Standard 170 defines specific occupied and unoccupied requirements by room type — and protective environment rooms, for example, do not permit airflow turndown. In these zones, redundancy means dual-fan configurations, backup power feeds, and failover controls — not optional upgrades, but baseline design criteria.
Regulatory Standards Every Healthcare Facilities Manager Must Know
Before specifying a single piece of equipment, facilities managers need a working understanding of the standards that govern healthcare ventilation.
ASHRAE Standard 170
ANSI/ASHRAE/ASHE Standard 170-2025 is the controlling benchmark for healthcare HVAC. It specifies requirements for a wide range of clinical and support spaces, covering nine variables per room type:
- Pressure relationship
- Outdoor air changes per hour
- Total ACH
- Exhaust requirements
- Room recirculation restrictions
- Filter efficiency
- Relative humidity range
- Temperature range
A room-by-room audit against Standard 170 must happen in the pre-procurement phase, not after equipment is specified. Retrofitting to compliance is far more expensive than planning for it.
Supporting Standards and Guidance
Three additional sources shape compliance decisions:
- ASHRAE Standard 62.1 — The general ventilation and indoor air quality standard. Its fact sheet explicitly requires Standard 170 compliance for outpatient, ambulatory surgery, and support spaces in healthcare settings
- CDC Infection Control Guidelines — For airborne infection isolation rooms (AIIRs), CDC TB guidance requires negative pressure of at least 0.01 in. w.g. (2.5 Pa), a minimum of 12 ACH in new or renovated rooms, and direct outdoor exhaust — or HEPA filtration before any unavoidable recirculation
- 2026 FGI Codes for Planning and Design — The Facility Guidelines Institute's current code cycle, which contains minimum requirements intended for adoption and enforcement in construction and renovation projects
Joint Commission and CMS Environment of Care
Accredited hospitals face additional scrutiny under Joint Commission EC.02.05.01, which specifically evaluates air pressure, filtration, and ACH in critical care areas. The Joint Commission's own survey guidance flags recurring findings in pressure control, temperature, humidity, and maintenance documentation. CMS Conditions of Participation layer on top of this, with compliance tied directly to Medicare and Medicaid participation.
Maintenance records, filter change logs, and pressure test results aren't just operational paperwork. In a Joint Commission or CMS audit, they're your primary evidence of compliance.
Filtration: The Most Critical — and Most Misunderstood — Component
Filter selection is where well-intentioned facilities managers most often create problems.
Understanding MERV Ratings
MERV (Minimum Efficiency Reporting Value) rates how effectively a filter captures particles between 0.3 and 10 microns across three size ranges under ANSI/ASHRAE 52.2. Higher MERV means finer filtration — but also higher airflow resistance (static pressure drop). This creates a core tension in healthcare: maximum particle capture vs. adequate airflow that doesn't strain the system.
The Common Specification Mistake
Selecting the highest available MERV filter without checking the system's designed CFM and static pressure tolerances is a frequent and costly error. A filter that's too restrictive for the air handler will:
- Reduce airflow below required ACH minimums
- Force fan motors to work harder, increasing energy consumption
- Shorten system lifespan
- Create compliance failures, not prevent them
Always verify filter performance at the system's actual operating face velocity. If a manufacturer's data sheet doesn't specify the test velocity alongside pressure drop figures, the numbers aren't comparable.
The Electronic Filtration Alternative
Electronic air cleaners (EACs) resolve the core tension between filtration efficiency and pressure drop. Instead of capturing particles by physically blocking them with a dense weave — which increases resistance as the filter loads — electronic filtration uses an electrostatic charge to attract particles to the media.
ECOairflow's M-Series Hybrid uses patented Electronic Polarization Technology (EPT) to achieve this. Key performance specifications:
- MERV 13A–16A certified under ASHRAE 52.2, including Appendix J in-situ protocol
- Pressure drop: 0.09–0.18 in.w.c. at 300 FPM — compared to 0.6–1.2 in.w.c. for a conventional MERV 8 pre-filter + MERV 14 bag filter train
- Maintains full rated MERV performance whether powered, unpowered, or under Appendix J conditioning — a critical distinction for medical treatment rooms where power interruptions cannot create filtration gaps
- UL 2998 Zero Ozone Verified (below 0.0005 ppm) — exceeds ASHRAE 170 emission standards for both ozone and formaldehyde, making it safe for ORs, ICUs, and protective environment rooms

A 12-week independent study comparing the M-Series against a traditional ASHRAE 170-compliant MERV 8 + MERV 14 bag filter configuration documented a 54% reduction in fan power consumption.
Room-Specific Filtration Requirements
Filtration strategy must be room-specific:
- Operating rooms — Positive pressure, MERV-16A minimum. M-Series MERV 16A pad is the specified ECOairflow configuration
- Airborne infection isolation rooms — Negative pressure, MERV-14 supply, direct outdoor exhaust. When HEPA is required upstream, the M-Series MERV 14A replaces the conventional MERV 8 + MERV 14 pre-filter stage
- Protective environment rooms — Positive pressure, HEPA-filtered supply. M-Series serves as the consolidated pre-filter, eliminating the two-bank pre-filter array while maintaining compliance
Filtration Evaluation Checklist
Before specifying any filter for a clinical zone:
- Confirm MERV rating is tested under ASHRAE 52.2 at the correct face velocity
- Verify performance under Appendix J in-situ conditioning, not just new-filter lab conditions
- Check whether the filter technology generates ozone or chemical byproducts in patient-occupied zones
- Calculate total annual cost: replacement frequency × unit cost, plus energy impact of pressure drop
- For electronic air cleaners, confirm powered, unpowered, and Appendix J performance are all documented
Air Pressure Control and Room Zoning Requirements
Positive vs. Negative Pressure — in Plain Language
- Negative pressure rooms (isolation rooms, AIIRs) exhaust more air than they supply. When a door opens, air flows inward from the hallway, keeping contaminated air contained inside the room.
- Positive pressure rooms (ORs, protective environment rooms) supply more air than they exhaust. When a door opens, air flows outward, preventing corridor contaminants from entering the sterile space.
Maintaining these differentials continuously is a life-safety function. The CDC-recommended minimum differential for AIIR rooms is 0.01 in. w.g. (2.5 Pa), verified by direct pressure measurement or smoke testing.
Zoning Design and Verification
Healthcare HVAC systems map pressure relationships between adjacent spaces (room → anteroom → hallway) to create deliberate airflow cascades that prevent cross-contamination. These cascades must be verified through actual pressure testing, not assumed from design specifications.
CDC verification cadence for TB isolation rooms:
- Occupied rooms: Visual verification required daily
- Unoccupied rooms: Monthly verification when not in active TB isolation use
Building automation systems (BAS) with continuous pressure monitoring can flag deviations automatically, giving facilities a real-time compliance record rather than relying on periodic manual checks alone.
Energy Efficiency, Redundancy, and Total Cost of Ownership
The Energy Reality
According to the U.S. Department of Energy, HVAC can account for nearly half of a hospital's total energy use — driven largely by the substantial outdoor air requirements that clinical spaces demand around the clock. Efficiency ratings quoted by manufacturers reflect ideal test conditions. Real-world performance depends on climate, building envelope, ductwork routing, and actual load — so model energy costs under realistic operating assumptions.
Reserve Capacity for Critical Zones
ASHRAE Addendum k to Standard 170 requires that central heating and cooling sources serving healthcare facilities maintain reserve capacity sufficient to sustain operations when one source or accessory fails. Essential accessories include failure-prone components like pumps, fans, and control-air compressors. Fan wall configurations are one practical approach: they allow one fan to fail without losing serviceability to the zone it serves.
Filtration as a TCO Factor
Filters with high pressure drop force HVAC fans to work harder — continuously, every day the system runs. The numbers matter at scale:
- Conventional hospital filter trains (MERV 8 pre-filter + MERV 14 bag): 0.6–1.2 in. w.c. pressure drop, with resistance increasing 60%+ as the filter loads over a 12-week cycle
- ECOairflow M-Series: 0.13–0.37 in.w.c., with pressure drop remaining nearly constant throughout the pad's service life
The M-Series' patented single-pad design also eliminates the Stage 2 bag filter array entirely, reducing both maintenance labor and the number of filter change touchpoints in clinical spaces. In environments where filter changes require infection control coordination, that reduction in touchpoints is a direct operational cost factor.
For capital planning conversations, facilities managers can contact ECOairflow directly at 1-877-347-3569 or customerservice@ecoairflow.com to request submittal documentation, Appendix J certification data, and ASHRAE 170/241 compliance documentation.
Building a Healthcare HVAC Maintenance Strategy
Core Components of a Compliant Program
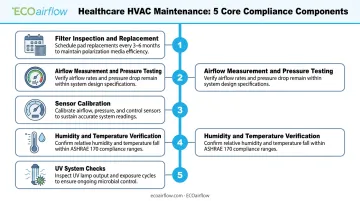
A maintenance program that holds up to Joint Commission and CMS scrutiny includes:
- Filter inspection and replacement on zone-specific schedules — not a building-wide calendar. For commercial and hospital-grade pads, ECOairflow recommends 3–6 months, with timing driven by particulate load rather than elapsed time
- Airflow measurement and pressure testing — to verify ACH and pressure differentials meet ASHRAE 170 room specifications
- Sensor calibration — temperature and humidity sensors drift; uncalibrated sensors produce false compliance readings
- Humidity and temperature verification against ASHRAE 170 zone classifications
- UV system checks where applicable
Facilities in high-particulate environments — near heavy traffic corridors, agricultural areas, or wildfire-prone regions — should use measured differential pressure and manufacturer service-limit thresholds to drive replacement timing, rather than a fixed calendar that ignores actual filter loading.
Each of these activities only counts if it's documented — which is where many facilities fall short.
The Documentation Imperative
Accurate, timestamped records of every maintenance activity — visual inspections, airflow measurements, filter changes, pressure tests — support Joint Commission EC.02.05.01 compliance, CMS Environment of Care audits, and potential legal defense.
Documentation gaps are among the most commonly cited findings in facility surveys. What you measured, when, and how becomes the evidence auditors examine.
ECOairflow provides ASHRAE 170/241 compliance documentation, Appendix J certification data, and product submittal sheets on request — materials that directly support the filter-related evidence categories auditors examine.
Frequently Asked Questions
What is HVAC in healthcare?
Healthcare HVAC refers to heating, ventilation, and air conditioning systems specifically designed and regulated for medical facilities. Unlike commercial systems, healthcare HVAC must control air pressure differentials, pathogen containment, humidity, and multi-tier filtration to protect patients, staff, and sterile environments — governed primarily by ASHRAE Standard 170.
What is the $5,000 rule for HVAC?
The $5,000 rule is a homeowner repair-vs-replace guideline: multiply the system's age by the estimated repair cost, and if the result exceeds $5,000, replacement is often more economical. No ASHRAE, FGI, CMS, or Joint Commission standard applies this rule to healthcare settings — where reliability, redundancy, and compliance requirements make lifecycle decisions considerably more complex.
What are the three types of HVAC systems?
The three common categories are split systems (separate indoor and outdoor units), packaged systems (all components in one unit), and variable refrigerant flow (VRF) systems. Healthcare facilities use combinations of these alongside specialized air handling units — but the applicable design standard is ASHRAE 170, which governs ventilation, filtration, pressure, and redundancy regardless of equipment type.
What MERV rating is required for hospital HVAC systems?
Requirements vary by room type under ASHRAE Standard 170:
- General exam rooms: MERV-8 minimum
- Airborne infection isolation rooms: MERV-14 supply filtration
- Operating rooms: MERV-16A
- Protective environment rooms: HEPA-filtered supply air, a distinct efficiency class that exceeds the MERV scale
What is the difference between positive and negative pressure rooms?
Negative pressure rooms (used for infectious isolation) exhaust more air than they supply, so airflow moves inward, containing pathogens within the room. Positive pressure rooms (used for ORs and immunocompromised patient care) supply more air than they exhaust, pushing air outward to prevent outside contaminants from entering.
How often should healthcare HVAC filters be replaced?
Replacement frequency depends on filter type, room classification, and environment — a single building-wide calendar rarely fits. Track differential pressure against manufacturer service limits and set zone-specific schedules for high-acuity areas.