Introduction
According to the EPA, Americans spend roughly 90% of their time indoors — and indoor air concentrations of some pollutants run 2 to 5 times higher than outdoor levels. When viruses like influenza and SARS-CoV-2 spread through respiratory aerosols in crowded, poorly ventilated spaces, indoor air quality stops being a comfort issue and becomes a genuine health concern.
HEPA filters are tested to capture 99.97% of particles at 0.3 microns and are widely deployed in hospitals, operating rooms, and residential HVAC systems. But a persistent question follows them: can they actually stop viruses? Most respiratory viruses measure under 0.3 microns — smaller than HEPA's rated benchmark — which leads many people to assume the answer is no. That assumption is wrong, though the full picture is more nuanced than a simple yes or no.
Understanding where that nuance lives — in capture physics, real-world testing, and the boundaries of what HEPA can and can't do — is what this guide covers.
Key Takeaways
- HEPA filters capture 99.97% of particles at 0.3 microns, but viruses are smaller — diffusion physics is what makes HEPA still effective against them
- Viruses travel on larger respiratory droplets that HEPA does capture effectively
- Diffusion mechanics make HEPA surprisingly good at trapping very small free-floating particles too
- HEPA traps viruses — it does not kill them; handling used filters carefully matters
- Real-world effectiveness depends heavily on room sizing, CADR ratings, placement, and continuous operation
What Is a HEPA Filter, and Why Are Viruses a Unique Challenge?
The HEPA Standard, Defined Precisely
Under U.S. standards (IEST), a true HEPA filter must capture a minimum of 99.97% of airborne particles at 0.3 microns. Under European standards (EN 1822:2019), H14-grade HEPA reaches 99.995%. These are tested, standardized ratings — not marketing claims.
The 0.3-micron benchmark isn't arbitrary. It represents the Most Penetrating Particle Size (MPPS) — the size at which particles are hardest to capture. Counterintuitively, both larger and smaller particles are captured more efficiently than particles at exactly 0.3 microns, because different physical mechanisms dominate at different size ranges.
Where Viruses Fit
Common respiratory viruses are genuinely small:
- Influenza virions: ~80–120 nm (0.08–0.12 microns)
- SARS-CoV-2: approximately 100 nm without spike proteins
- Adenovirus: ~95 nm
All of these fall below the 0.3-micron HEPA benchmark — which leads to the common misconception that HEPA filters can't catch them.
HEPA is not a sieve. It doesn't simply block particles larger than 0.3 microns and let smaller ones through. The filter captures particles across a wide size range through multiple physical mechanisms — including diffusion, interception, and inertial impaction — each of which becomes more effective at the sub-0.3-micron range where viruses live. Understanding those mechanisms explains why virus-sized particles are actually captured more reliably than the MPPS benchmark suggests.
How HEPA Filters Capture Viruses: The Mechanics
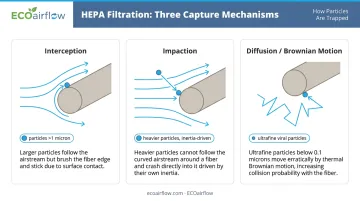
HEPA filtration uses three distinct physical capture mechanisms. Each one dominates at a different particle size range, and together they cover the full spectrum.
Interception and Impaction (Larger Particles)
Interception occurs when a particle following an airstream passes close enough to a fiber to adhere to it. Impaction occurs when heavier particles carry enough inertia that they can't follow the curving airstream around a fiber and collide directly with it.
Both mechanisms work best on particles larger than ~1 micron. This is where respiratory droplets fall — and that matters enormously.
Respiratory viruses don't typically travel as free-floating individual particles. They travel embedded in droplets expelled during coughing, sneezing, and talking. Research on speech droplet physicochemistry shows droplet count median diameters in the range of 1.6 and 2.5 microns — well within HEPA's interception and impaction range. Larger oral-cavity droplets go even higher. This is the primary reason HEPA works against airborne viral transmission despite virus particles themselves being sub-micron.
Diffusion and Brownian Motion (Ultrafine Particles)
Below ~0.1 microns, particles become too small to follow predictable airstream paths. Instead, they zigzag erratically due to collisions with air molecules — a phenomenon called Brownian motion.
That erratic behavior increases the probability of fiber contact and capture. Free-floating viral particles in this size range are often captured more effectively than mid-range particles because of this diffusion effect. Once particles contact a fiber, van der Waals forces — chemical adhesion — keep them anchored there.
The practical implication: HEPA's efficiency curve actually rises again for very small particles, so free-floating viruses below 0.1 microns are not left unaddressed.
Beyond Passive HEPA: Electronic Polarization
Some systems add an active electrical layer on top of fiber mechanics. ECOairflow's filtration products use Electronic Polarization Technology (EPT), which charges both particles and filter fibers, increasing attraction across all particle sizes. Independent lab testing shows ECOairflow's Model 2300 captures 74.73% of PM0.1 ultrafine particles, compared to HEPA's 49.19%, making it 50% more effective in that sub-0.1-micron range where free-floating viral particles reside.
How Well Do HEPA Filters Actually Work Against Viruses?
What the Research Shows
A 2021 systematic review published in Otolaryngology–Head and Neck Surgery found experimental evidence that portable HEPA purifiers can reduce or eliminate airborne SARS-CoV-2 and surrogates in indoor settings. Multiple studies support HEPA's ability to meaningfully reduce airborne viral concentrations.
Reducing viral concentration in the air, however, is not the same as preventing infection.
A December 2023 review in Preventive Medicine analyzed 32 studies and found no clear net benefit from air filtration for actual infection outcomes. The gap exists for practical reasons:
- Close-contact transmission happens before filtered air can intervene
- Direct droplet exposure at short range bypasses the filtration cycle entirely
- Individual exposure variation makes population-level infection outcomes hard to attribute to filtration alone
This distinction matters when setting realistic expectations for what filtration alone can accomplish.
The Variables That Actually Determine Performance
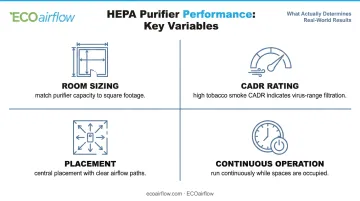
Filter grade is only part of the picture. Real-world effectiveness depends on:
- Room sizing — An undersized unit recirculates air too slowly. Match the purifier's capacity to the actual square footage of the space
- CADR rating — The EPA recommends choosing units with a high CADR for tobacco smoke, which indicates capacity to filter the smallest particles including virus-range aerosols
- Placement — Units placed against walls or in corners have reduced airflow efficiency; central placement with clear airflow paths performs significantly better
- Continuous operation — The EPA recommends running air purifiers continuously while spaces are occupied, not intermittently
Air Changes Per Hour (ACH)
These variables — room size, CADR, and runtime — all feed into a single measurable outcome: ACH, or air changes per hour. ACH describes how many times per hour the full volume of room air passes through the filter, and it's the most direct measure of how quickly a system reduces airborne viral load.
The CDC's infection control data illustrates the difference clearly: at 6 ACH, achieving 99% airborne contaminant removal takes approximately 46 minutes. At 12 ACH, the same result takes about 23 minutes. ASHRAE Standard 170 specifies 20 total ACH for hospital operating rooms. Residential settings typically achieve far lower ACH — which is why sizing and continuous operation matter so much.
What HEPA Filters Cannot Remove
Viruses Are Trapped, Not Destroyed
HEPA filters trap viral particles in their fiber matrix — they do not inactivate or kill them. Captured viruses can remain viable depending on the strain and surface conditions:
- SARS-CoV-2 in aerosols: viable for up to 3 hours (NIH data)
- Influenza A on hard nonporous surfaces: survives 24–48 hours
- Influenza on cloth/paper: less than 8–12 hours
Virus viability on dry HEPA filter media hasn't been directly measured in controlled published studies — results vary by strain. What is established: proper filter handling matters. Use gloves during replacement and seal used filters before disposal.
What HEPA Physically Cannot Capture
HEPA filters have no effect on:
- Gases and VOCs — chemical fumes, volatile organic compounds, and odors are molecular in scale, not particulate; they pass through fiber media entirely and require activated carbon filtration
- Radon gas — particulate filtration doesn't address gas-phase radon; radon-specific mitigation is required
- Contact transmission — HEPA provides no protection against fomite transmission or direct physical contact with contaminated surfaces
The Re-Release Question
Some concern exists about whether captured particles can be dislodged from HEPA filters. Research on particle re-entrainment from loaded HEPA filters (including a study on captured plutonium particles) confirms that re-entrainment can occur, particularly under high airflow, reverse-airflow conditions, or significant filter loading.
Under normal forward airflow conditions, re-release appears minimal. Practical guidance for safe handling:
- Avoid handling used filters carelessly or shaking them out
- Never re-insert a filter in reverse orientation
- Replace filters on schedule before excessive loading occurs
Where High-Efficiency Air Filtration Makes the Most Difference
High-Impact Settings
Some environments see the greatest measurable benefit from high-efficiency filtration:
- Hospitals and clinical spaces — CDC and ASHRAE Standard 170 specify HEPA use in certain protective environment rooms; operating rooms require 20 total ACH; immunocompromised patients face the highest stakes from airborne pathogen exposure
- Schools and offices — A 2023 scoping review confirmed ventilation meaningfully reduces airborne infection risk in schools by reducing the residence time of infectious aerosols; CO2 monitoring serves as a useful proxy for ventilation adequacy
- High-traffic facilities — Dense, mixed populations with continuous air recirculation create conditions where filtration efficiency has compounding effect on overall exposure reduction
Facilities like these require filtration systems that meet strict regulatory thresholds — not just adequate ones. ECOairflow's electronic air filtration systems are deployed in hospitals, airports, and casinos across North America. The M-Series Hybrid carries MERV 13–16 certification (Appendix J certified under ASHRAE 52.2), full ASHRAE 170 / CSA Z317.2 hospital compliance, and ETL-listed UL 2998 Zero Ozone certification — important in healthcare settings where ozone-generating equipment creates its own patient safety risk.

Practical Guidance for Residential Users
HEPA filtration delivers the most benefit:
- In bedrooms — where people spend the most consecutive hours and extended close exposure occurs during sleep
- In homes with immunocompromised individuals — where marginal reduction in viral load matters more than in healthy households
- During flu season or active illness — where household members are shedding virus and close-contact risk is highest
Running units continuously at appropriate fan settings — not just when someone feels sick — is what converts filter grade into measurable air quality improvement.
Frequently Asked Questions
Do HEPA filters remove viruses?
Yes, HEPA filters capture viruses — primarily because viruses travel on larger respiratory droplets that fall within HEPA's interception range, and because diffusion mechanics capture very small free-floating particles too. They reduce airborne viral concentration meaningfully but do not eliminate infection risk entirely.
What do HEPA filters not remove?
HEPA filters cannot capture gases, VOCs, chemical odors, or radon — these require activated carbon or radon-specific mitigation technologies. HEPA also provides no protection against contact-based (fomite) transmission or direct respiratory droplet exposure at close range.
Do HEPA filters kill viruses or just trap them?
HEPA filters trap viruses in their fiber matrix but do not destroy them. Virus viability on filter surfaces varies by strain and conditions. When replacing filters, wear gloves and seal used filters before disposal to minimize handling risk.
Are HEPA filters effective against COVID-19?
Peer-reviewed studies show HEPA-equipped air purifiers measurably reduce airborne SARS-CoV-2 concentrations, particularly when properly sized and run continuously. However, filtration alone is not sufficient protection against COVID-19 and works best as one layer in a broader infection control approach.
What MERV rating do you need to filter viruses from air?
The EPA recommends MERV 13 or higher for HVAC systems to capture virus-range particles effectively. HEPA filters exceed this — CDC/NIOSH confirms HEPA is more efficient than MERV 16 for human-generated infectious particles. Standard MERV 8–11 filters common in residential systems are not rated for virus-sized particles.
How often should a HEPA filter be replaced to maintain virus protection?
Most manufacturers recommend replacement every 6–12 months under normal use. A clogged or degraded filter reduces airflow and overall device effectiveness. In high-occupancy or health-sensitive settings, inspecting filters more frequently and replacing proactively is the safer approach.